Lisinopril
Buy 5 mg lisinopril with mastercardThe usefulness of immunofluorescent tests in pemphigus sufferers in clinical remission pulse pressure 43 lisinopril 10 mg purchase without prescription. Pemphigus in remission: Value of unfavorable direct immunofluorescence in management blood pressure medication and weight loss 5 mg lisinopril cheap free shipping. Value of direct immunofluorescence in predicting arrhythmia when falling asleep generic lisinopril 10 mg fast delivery, remission in pemphigus vulgaris. The use of two substrates to enhance the sensitivity of indirect immunofluorescence in the diagnosis of pemphigus. Pemphigus vulgaris: Superior sensitivity of monkey esophagus within the determination of pemphigus antibody. The use of two substrates for indirect immunofluorescence within the prognosis of pemphigus: Reply from authors. The use of two substrates for indirect immunofluorescence in the analysis of pemphigus. Anti-intercellular substance antibodies: Presence in serum samples of 14 sufferers with out pemphigus. Reflectance confocal microscopy as a model new device in the in vivo analysis of desquamative gingivitis: Patterns in mucous membrane pemphigoid, pemphigus vulgaris and oral lichen planus. Ultrastructural examine of clinically uninvolved skin of sufferers with pemphigus vulgaris. The location of binding sites of pemphigus vulgaris, and pemphigus foliaceus autoantibodies: A post-embedding immunoelectron microscopic examine. Pemphigus vegetans: Its relationship to eosinophilic spongiosis and favorable response to dapsone. Pyodermite v�g�tante of Hallopeau: Immunofluorescence studies performed in an early disease stage. Pemphigus vegetans with oesophageal involvement: Successful treatment with minocycline and nicotinamide. Pyodermatitis�pyostomatitis vegetans: A specific marker for inflammatory bowel disease. Pyodermatitis�pyostomatitis vegetans: Evidence for a completely mucocutaneous variant. Pyodermatitis�pyostomatitis vegetans complicated by methicillin-resistant Staphylococcus aureus an infection. Pyostomatitis vegetans: Dramatic clinical response to clobetasol propionate treatment in aqueous solution. Pyodermatitis�pyostomatitis vegetans: A scientific course of two decades with response to cyclosporine and low-dose prednisolone. Three instances of pemphigus vegetans: Induction by enalapril � Association with internal malignancy. Epidermal antigens and complement-binding anti-intercellular antibodies in pemphigus vegetans, Hallopeau type. Pyodermatitis�pyostomatitis vegetans with circulating autoantibodies to bullous pemphigoid antigen 230. Ultrastructural morphometry of normal human dermal� epidermal junction: the influence of age, intercourse, and physique area on laminar and nonlaminar elements. Anti-basement membrane, autoantibodies in patients with anti-epiligrin cicatricial pemphigoid bind the subunit of laminin 5. Plasmin induces degradation and dysfunction of laminin 332 (laminin 5) and impaired assembly of basement membrane on the dermal�epidermal junction. Focal dermal�epidermal separation and, fibronectin cleavage in basement membrane by human mast cell tryptase. Inherited epidermolysis bullosa: Clinical options, molecular genetics, and pathoetiologic mechanisms. Ultrastructural clues to genetic problems of skin: the dermal�epidermal junction. Assessment of mobility, activities and pain in numerous subtypes of epidermolysis bullosa. Overview of the Proceedings of the 2nd International Symposium on Epidermolysis Bullosa, Santiago, Chile, 2005. Clinicopathologic forms of epidermolysis bullosa and their nondermatological complications. Revised clinical and laboratory criteria for subtypes of inherited epidermolysis bullosa. The basement membrane: Interface between the epithelium and the dermis � Structural options. Antigenic features and structural correlates of basement membranes: Relationship to epidermolysis bullosa. Physicochemical characterization and differentiation of the components of the cutaneous basement membrane zone. Age-related practical and structural adjustments in human dermo-epidermal junction elements. A comparative research of immunohistochemistry and electron microscopy used within the diagnosis of epidermolysis bullosa. A comparative examine between transmission, electron microscopy and immunofluorescence mapping within the prognosis of epidermolysis bullosa. Inherited epidermolysis bullosa comes into the model new millennium: A revised classification system primarily based on current knowledge of pathogenetic mechanisms and the clinical, laboratory, and epidemiologic findings of large, well-defined patient cohorts. Revised classification system for inherited epidermolysis bullosa: Report of the Second International Consensus Meeting on Diagnosis and Classification of Epidermolysis Bullosa. Generalized dominant epidermolysis bullosa simplex: Decreased exercise of a gelatinolytic protease in cultured fibroblasts as a phenotypic marker. Partial dominance of a keratin 14 mutation in epidermolysis bullosa simplex � Increased severity of illness in a homozygote. Lethal epidermolytic epidermolysis bullosa: A new autosomal recessive type of epidermolysis bullosa. Partial revertant mosaicism of keratin 14 in a patient with recessive epidermolysis bullosa simplex. Successful prenatal exclusion of an unspecified subtype of extreme epidermolysis bullosa. Analysis of skin-derived amniotic fluid cells within the second trimester; Detection of severe genodermatoses expressed within the fetal period. Homozygosity mapping as a screening tool for the molecular prognosis of hereditary skin ailments in consanguineous populations. Generation and characterization of epidermolysis bullosa simplex cell lines: Scratch assays present sooner migration with disruptive keratin mutations. A common keratin 5 gene mutation in, epidermolysis bullosa simplex � Weber�Cockayne. Genetic bases of epidermolysis bullosa simplex and, epidermolytic hyperkeratosis. Mutations within the genes for epidermal keratins in epidermolysis bullosa and epidermolytic hyperkeratosis. The molecular genetics of the genodermatoses: Progress to date and future instructions. Epidermolysis bullosa simplex in Japanese and Korean patients: Genetic research in 19 cases. Keratin 14 point mutations at codon 119 of helix 1A leading to different epidermolysis bullosa simplex phenotypes. A novel mutation in the L12 area of keratin 5, in the K�bner variant of epidermolysis bullosa simplex. Localized epidermolysis bullosa simplex with generalized enamel hypoplasia in a toddler. DesGroseilliers J-P Brisson P Localized epidermolysis bullosa: Report of two cases and. Epidermolysis bullosa simplex: Identification of a kindred with autosomal recessive transmission of the Weber�Cockayne selection. Novel K5 and K14 mutations in German patients with the Weber�Cockayne variant of epidermolysis bullosa simplex. A new keratin 5 mutation (K199T) in a household with Weber�Cockayne epidermolysis bullosa simplex. A new mutation within the linker 12 area of keratin 5 in a Chinese household with Weber�Cockayne epidermolysis bullosa simplex. Tetracycline and epidermolysis bullosa simplex: A new indication for one of the oldest and most widely used medication in dermatology
5 mg lisinopril purchase otcCauses of Thrombocytopenia During Pregnancy Acute fatty liver of pregnancy Antiphospholipid syndrome and systemic lupus erythematosus Marrow issues blood pressure 9040 2.5 mg lisinopril discount with mastercard. A dose of 1 g/kg per day for 2 days hypertension 5 mg lisinopril 5 mg buy discount online, or 400 mg/kg per day for 5 days can be used alone blood pressure chart 80 year old 5 mg lisinopril generic visa, or mixed with low-dose prednisone. These research reported that publicity to these medication during being pregnant was not associated with a rise within the risk of unfavorable pregnancy outcomes and had no important toxicity to the fetus. It can cross the placenta, and switch from mom to fetus increases with gestational age. The half-life of the drug can also be very lengthy; rituximab can be found in blood 6 months after of an infusion. This retrospective examine confirmed low risk of premature births, hematologic abnormalities and start defects. However, because of the dearth of managed research, it is strongly recommended that ladies keep away from being pregnant for 1 yr after rituximab infusion. During vaginal supply, the goal maternal platelet count must be 50 � 109/L or larger. If cesarean section or epidural anesthesia is required, the platelet count must be maintained over 70 to eighty � 109/L. If the new child is thrombocytopenic, the platelet count should be measured day by day for 1 week. Platelet transfusions and glucocorticoids are added if bleeding is life-threatening. Eclampsia is defined by the incidence of epileptic seizures in a preeclamptic girl during the peripartum period. During normal implantation, these cells convert from epithelial to endothelial morphology, a process called pseudovasculogenesis. A large volume of evidence implicates sFlt1 as enjoying a key position within the pathogenesis of preeclampsia. Its expression in rats produces a syndrome akin to preeclampsia: hypertension and proteinuria related to glomerular endotheliosis (occlusion of glomerular capillaries by swollen endothelial cells). However, thrombocytopenia is more common in preterm infants, of a quantity of potential etiologies. Severe thrombocytopenia (<50 � 109/L) is a vital discovering in neonates, and should be rigorously managed because of high bleeding threat (Chap. In both illnesses, maternal alloantibodies in opposition to fetal blood cell antigens cross the placenta and destroy antigen-positive fetal cells, resulting in important fetal/ neonatal morbidity and mortality. This syndrome occurs in the peripartum period and is outlined by the presence of microangiopathic hemolytic anemia, elevated liver enzymes, and low platelets. Adhesion and aggregation of platelets on broken and activated endothelium presumably accounts for the low platelet count (Chap. Six or extra of these standards should be current in a affected person who has no obvious cause for hepatic failure. Both maternal and fetal mortality charges are high, ranging from 7 to 18 percent and 9 to 23 p.c, respectively. The platelet rely nadir and the peak of serum lactate dehydrogenase may occur postpartum, during the first postpartum day in most sufferers, however as late as 5 to 7 days in some. In extreme circumstances, intracranial hemorrhage and hydrocephalus could develop and cause fetal dying or severe neurologic sequelae. Ultrasonography is normally not useful until it detects bleeding or hydrocephalus. Bleeding could also be delayed, because the platelet count normally falls further through the first a quantity of days of life. Matched platelet transfusions will only transiently enhance the fetal platelet rely because the transfused platelets also are targeted by the offending antibodies. Thus, the total blood platelet pool in a affected person with splenomegaly might be normal even when the counts measured in venous blood are solely 20 % of regular. Platelet manufacturing is usually regular in patients with splenomegaly, as estimated by dividing the whole body platelet mass by the platelet life span. The most typical disorder inflicting thrombocytopenia due to splenic pooling is continual liver disease with portal hypertension and congestive splenomegaly. In sufferers with cirrhosis and portal hypertension, moderate thrombocytopenia is the rule. Signs and signs are associated to the primary disorder, and bleeding manifestations result primarily from coagulation abnormalities attributable to the underlying liver disease. This finding is in keeping with the relatively average diploma of thrombocytopenia, the near-normal total body content material of platelets,370 and the flexibility to mobilize platelets from the spleen to replenish losses. Magnetic resonance imaging defines the blood flow sample, which is particularly helpful for detecting portal or splenic vein thromboses. Cell survival studies using radiolabeled platelets or pink blood cells could be useful for identifying hypersequestration when weighing the need for splenectomy. Most sufferers with splenomegaly require therapy for the underlying illness quite than for thrombocytopenia. With no therapy apart from rewarming, platelet counts returned to normal in four to 10 days. On the other hand, Kaposi-like hemangioendothelioma and tufted angioma are low-grade malignant vascular tumors associated with excessive morbidity and mortality. Vascular tumors normally are solitary, can attain 20 cm in diameter, and could be superficial or invade internal organs and the retroperitoneum. The histologic types more incessantly related to Kasabach-Merritt syndrome are Kaposi-like hemangioendothelioma and tufted angiomas or angioblastomas. These tumors are composed predominantly of plump, round, oval, and/or spindled endothelial cells with hemosiderin deposits. Initial bodily entrapment of the platelets inside twisted abnormal vessels might favor their adhesion to abnormal endothelium, which may lead to platelet activation and aggregation followed by activation of the coagulation cascade, fibrin deposition, and formation of microthrombi. Excessive move and shear rates generated by arteriovenous shunting inside the tumor further improve the extent of platelet activation. Continuous thrombus formation results in platelet consumption and activation of the fibrinolytic cascade. Several particular therapeutic modalities have been proposed, but none has been established as persistently effective. One examine of sufferers requiring massive transfusion demonstrated that delicate thrombocytopenia (47 to a hundred � 109/L) occurred in all sufferers after transfusion of 15 purple cell units, and extra severe thrombocytopenia (25 to sixty one � 109/L) developed after 20 purple cell items. Massively transfused sufferers ought to be treated with fresh-frozen plasma to exchange coagulation elements, and with platelets. Thus, thrombocytopenia is less extreme in cardiac surgery sufferers supported by normothermic systemic perfusion (35�C to 37�C) than in these supported by reasonably hypothermic systemic perfusion (25�C to 29�C). The mortality fee for advanced Kasabach-Merritt syndrome is roughly 12 percent; the speed is larger when associated with retroperitoneal or intraabdominal tumors. This section discusses medicine, other than heparins, that cause isolated thrombocytopenia by immune platelet destruction; Chap. In reported cases, the median nadir and peak platelet counts have been 10 � 109/L (range: 1 to 90 � 109/L) and 330 � 109/L (range: 72 to 2300 � 109/L), respectively. The bleeding tendency ranges from asymptomatic, to simple bruising, gingival bleeding, recurrent epistaxis, menorrhagia, and hematuria, to more serious bleeding, together with gastrointestinal or central nervous system hemorrhage. In female patients, oral contraceptives could additionally be helpful to delay the menstrual cycle and cover low-platelet-count days. Antifibrinolytic medicine similar to aminocaproic acid or tranexamic acid may be helpful to lower bleeding signs. To address the difficulty of which drugs more than likely cause thrombocytopenia, a scientific evaluation of all revealed case stories defined ranges of proof to doc the causal relation between the drug and thrombocytopenia. Other commonly cited drugs are just like drugs documented in a case-control research. Drugs could bind covalently to membrane proteins, and should induce hapten-dependent antibodies in sufferers receiving penicillin and cephalosporin. In quinine-induced thrombocytopenia, antibodies bind to membrane proteins solely within the presence of soluble drug. Initial experimental observations advised that drug�antibody complexes bind to platelets via the platelet Fc receptor. Drugs must be thought of as potentially causative in any thrombocytopenic affected person on medication, taking herbal cures, or using iodinated radiocontrast solutions. Discontinuation of the causative drug(s) is the principle therapy technique; glucocorticoids could assist in some sufferers.
Cheap lisinopril 5 mg without prescriptionHyposensitization in nickel allergic contact dermatitis: Clinical and immunologic monitoring heart attack high dead end counterpart lisinopril 5 mg generic online. Effects of repeated skin publicity to low nickel concentrations: A mannequin for allergic contact dermatitis to nickel on the arms heart attack low 10 mg lisinopril order otc. Loss-of-function mutations in the filaggrin gene and allergic contact sensitization to nickel hypertension chart lisinopril 2.5 mg order free shipping. Decrease in nickel sensitization in a Danish schoolgirl inhabitants with ears pierced after implementation of a nickel-exposure regulation. Nickel sensitization in adolescents and affiliation with ear piercing, use of dental braces and hand eczema. Reactivity to euro coins and sensitization thresholds in nickel-sensitive topics. Nickel launch from earrings bought in the United States:, the San Francisco earring research. The impression of various patient factors on contact allergy to nickel, cobalt, and chromate. Utility of a standard allergen series alone within the analysis of allergic contact dermatitis: A retrospective examine of 732 patients. North American Contact Dermatitis Group patch check outcomes for the detection of delayed-type hypersensitivity to topical allergens. Patch testing with preservatives, antimicrobials and industrial biocides: Results from a multicentre research. A evaluation of 241 topics who were patch tested, twice: Could fragrance combine 1 cause active sensitization Allergic contact dermatitis: Correlation of in vivo confocal imaging to routine histology. Confocal histopathology of irritant, contact dermatitis in vivo and the impact of skin shade (black vs. Pilot research on the sensitivity and specificity of in vivo reflectance confocal microscopy in the diagnosis of allergic contact dermatitis. Antigen-presenting cell operate of epidermal cells activated by hapten software. The relationships between exposure dose and response in induction and elicitation of contact hypersensitivity in humans. Lymphocyte function-associated antigen-1 is required for optimum elicitation of allergic contact dermatitis. Human natural killer T cells infiltrate into the pores and skin at elicitation sites of allergic contact dermatitis. Analysis of the sign transduction pathway of nickel-induced matrix metalloproteinase-2 expression in the human keratinocytes in vitro: Preliminary findings. Interleukin-12 expression in human afferent lymph derived from the induction phase of allergic contact dermatitis. Changes in epidermal proliferation and differentiation in allergic and irritant contact dermatitis reactions. The differential destiny of cadherins throughout T-cell-induced keratinocyte apoptosis leads to spongiosis in eczematous dermatitis. The persistence of allergic contact sensitivity: A 10-year follow-up in one hundred patients. Free radicals in antigen formation: Reduction of contact allergic response to hydroperoxides by epidermal remedy with antioxidants. The use of dietary manipulation in patients referred to a contact dermatitis clinic. Evaluation of the histologic characteristics of patch take a look at confirmed allergic contact dermatitis. Propolis-induced granulomatous contact dermatitis accompanied by marked lymphadenopathy. Lymphomatoid contact dermatitis caused by isopropyl-diphenylenediamine: Two circumstances. Cutaneous pseudolymphoma, lymphomatoid, contact dermatitis type, as an unusual cause of symmetrical higher eyelid nodules. A follow-up: Previously reported obvious, lymphomatoid contact dermatitis, now followed by T-cell prolymphocytic leukaemia. Protein contact dermatitis in meals staff: Case report of a meat sorter and abstract of seven other cases. Identification of IgE-reactive proteins in sufferers with wheat protein contact dermatitis. Nummular eczema: An addition of senile xerosis and distinctive cutaneous reactivities to environmental aeroallergens. Severe, generalized nummular eczema secondary to interferon alfa-2b plus ribavirin mixture remedy in a affected person with persistent hepatitis C virus an infection. Methotrexate is a secure and efficient remedy for paediatric discoid (nummular) eczema: A case series of 25 children. On the idea of distinctive exudative discoid and lichenoid persistent dermatosis (Sulzberger�Garbe): Is it nummular dermatitis Retrospective study of intraepidermal nerve fiber distribution in biopsies of sufferers with nummular eczema. Distinctive exudative discoid and lichenoid continual dermatosis (Sulzberger and Garbe) re-examined � 1978. Exudative discoid and lichenoid continual dermatosis (Sulzberger�Garbe): A fictional disease T-cell subset assay: A useful differentiating marker of, atopic and seborrheic eczema in infancy Early diagnosis of childish seborrhoeic dermatitis and atopic dermatitis � Clinical options. Early diagnosis of infantile seborrhoeic dermatitis and atopic dermatitis � Total and specific IgE ranges. The frequency of common skin conditions in, preschool-aged kids in Australia: Seborrhoeic dermatitis and pityriasis capitis (cradle cap). Seborrheic-like dermatitis of acquired immunodeficiency syndrome: A clinicopathologic examine. Seborrheic dermatitis and atopic eczema in human immunodeficiency virus infection. Eczema-like lesions and disruption of therapy in sufferers handled with interferon-alfa and ribavirin for persistent hepatitis C: the value of an interdisciplinary assessment. Unilateral seborrheic dermatitis after decompression of Chiari I malformation and syringomyelia. Seborrhoeic dermatitis-like manifestation of lung most cancers evolving into erythrodermia. High prevalence of seborrhoeic dermatitis on the face and scalp in mountain guides. Pityriasis amiantacea, an unrecognized cause of scarring alopecia, described in 4 patients. Pityriasis amiantacea: A distinctive presentation of psoriasis associated with tumour necrosis factor-alpha inhibitor remedy. Dandruff is associated with disequilibrium within the proportion of the main bacterial and fungal populations. The carriage of Malassezia furfur serovars A, B and C in patients with pityriasis versicolor, seborrhoeic dermatitis and controls. Seborrhoeic dermatitis and Pityrosporum (Malassezia) folliculitis: Characterization of inflammatory cells and mediators in the skin by immunohistochemistry. Tinea versicolor with regard to seborrheic dermatitis: An epidemiological investigation. Quantitative pores and skin cultures of Pityrosporum yeasts in sufferers seropositive for the human immunodeficiency virus with and with out seborrheic dermatitis. Identification of Malassezia species from immunocompetent and immunocompromised patients with seborrheic dermatitis. Seborrhoeic dermatitis and Pityrosporum ovale: A cultural and immunological examine. Correlation of Pityrosporum ovale density with medical severity of seborrheic dermatitis as assessed by a simplified method.
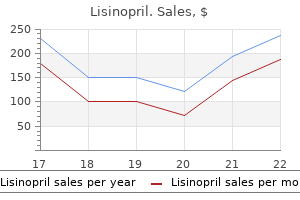
| Comparative prices of Lisinopril | | # | Retailer | Average price | | 1 | A&P | 340 | | 2 | PetSmart | 172 | | 3 | Giant Eagle | 286 | | 4 | Kroger | 814 | | 5 | Delhaize America | 428 | | 6 | Ross Stores | 503 | | 7 | Burlington Coat Factory | 642 | | 8 | Meijer | 631 |
Lisinopril 10 mg buy generic lineThe neutrophilic infiltrate is usually only gentle hypertension pregnancy discount 5 mg lisinopril otc, though there are numerous extravasated erythrocytes quitting high blood pressure medication discount lisinopril 2.5 mg on-line. The vessels in the underlying dermis present the typical options of an acute vasculitis blood pressure chart new zealand 5 mg lisinopril generic fast delivery. A vasculitis is normally present within the bullous lesions related to septicemia brought on by Vibrio vulnificus2448 and, rarely, by Escherichia coli,2449 Yersinia enterocolitica, and Morganella morganii. There is a heavy infiltrate of neutrophils in the higher and mid dermis, often with leukocytoclasis. The lesions vary in look from herpetiform vesicles to large hemorrhagic bullae. Nuclear dust is distinguished within the papillae and sometimes around superficial blood vessels. Infection might have been the precipitating explanation for two cases reported as IgE bullous disease. Rarely, this entity has developed in affiliation with different neurological disorders;2467 it adopted treatment with the -adrenergic antagonist atenolol in a affected person with pheochromocytoma. In this instance, direct immunofluorescence reveals linear IgG deposition alongside the dermal�epidermal junction. Penicillamine could produce blisters at completely different anatomical levels within the dermis, resembling both pemphigus foliaceus or pemphigus vulgaris. An uncommon bullous eruption has been reported in a patient receiving intravenous trimethoprim�sulfamethoxazole. On gentle microscopy they had been subepidermal with a light, mixed inflammatory cell infiltrate. Unusual blisters resembling bubble wrap developed after occupational skin damage with 35% hydrogen peroxide. There is focal necrosis of keratinocytes in and adjacent to the acrosyringium; generally the epithelium within the pilosebaceous follicles additionally exhibits focal necrosis. The basement membrane of the sweat glands may also be destroyed, but the myoepithelial cells often survive. Some arterioles show necrosis of their walls with a gentle perivascular infiltrate of neutrophils. The dermal infiltrate is composed of neutrophils, eosinophils, and a few lymphocytes. The mechanism remains to be determined, although the blisters apparently develop as a outcome of damage to the basal and suprabasal layers of the dermis. Histopathology2483 the cancer-related bullae with gyrate lesions are usually subepidermal in location, and the inflammatory cell infiltrate within the dermis is mild and of blended sort. Similar modifications have been reported following skin publicity to nitrogen and sulfur mustard. Interkeratinocyte adherens junctions: Immunocytochemical visualization of cell�cell junctional structures, distinct from desmosomes, in human epidermis. Relationship of adhesion molecules expression with epithelial differentiation markers throughout fetal pores and skin growth. Pemphigus sera recognize, conformationally sensitive epitopes in the amino-terminal region of desmoglein-1. The distribution of sixty four integrins in lesional and non-lesional pores and skin in bullous pemphigoid. Clinical and immunological heterogeneity, of canine subepidermal blistering dermatoses with anti-laminin-332 (laminin-5) autoantibodies. Displacement of desmoplakin from cell�cell interfaces disrupts anchorage of intermediate filament bundles and alters junction meeting. Identification of a 450-kDa human epidermal autoantigen as a model new member of the plectin family. Peristomal and generalized bullous pemphigoid in sufferers with underlying inflammatory bowel disease: Is plectin the missing hyperlink Differential expression of desmosomal plakophilins in numerous kinds of carcinomas: Correlation with cell kind and differentiation. Skin fragility and hypohidrotic ectodermal dysplasia resulting from ablation of plakophilin 1. Immunofluorescence on cut up pores and skin for the detection and differentiation of basement membrane zone autoantibodies. Autoimmune blistering illnesses: An update of diagnostic strategies and investigations. Ultrastructural evidence for using NaCl-split skin in the evaluation of subepidermal bullous illnesses. Clinical, histologic, and immunopathologic comparability of pemphigus vulgaris and pemphigus foliaceus. Clinical and immunological profile of umbilical involvement in pemphigus vulgaris and pemphigus foliaceus. Transplacental passage of maternal pemphigus foliaceus autoantibodies induces neonatal pemphigus. Generalized erythrodermic pemphigus foliaceus in a toddler and its profitable response to rituximab treatment. Pemphigus foliaceus in young women: An endemic, focus in the Sousse space of Tunisia. A case of herpetiform pemphigus related to autoimmune hemolytic anemia: Detection of autoantibodies towards multiple epidermal antigens. Pemphigus herpetiformis is a uncommon medical expression of nonendemic pemphigus foliaceus, fogo selvagem, and pemphigus vulgaris. Theopronine-induced herpetiform, pemphigus: Report of a case studied by immunoelectron microscopy and immunoblot evaluation. Development of pemphigus vulgaris in a patient with pemphigus foliaceus: Antidesmoglein antibody profile shift confirmed by enzyme-linked immunosorbent assay. Clinical proof of an intermolecular epitope spreading in a patient with pemphigus foliaceus converting into bullous pemphigoid. Changes within the autoimmune blistering response: A clinical and immunopathological shift from pemphigus foliaceus to bullous pemphigoid. Pemphigus with features of each vulgaris and foliaceus variants, related to antibodies to a hundred and sixty and 130 kDa antigens. Pemphigus with clinical, histological and, immunological features of both vulgaris and foliaceus subtypes. Combined features of pemphigus foliaceus and bullous pemphigoid: Immunoblot and immunoelectron microscopic research. Pemphigus foliaceus in an 11-year-old boy with dermatomyositis: Simple coincidence or familial immunological background Pemphigus foliaceus coexisting with IgA nephropathy in a patient with psoriasis vulgaris. Thyroid gland tumour, pemphigus foliaceus and myasthenia gravis within the daughter of a woman with myasthenia gravis. Pemphigus foliaceus and oral lichen planus in a affected person with systemic lupus erythematosus and thymoma. Pemphigus foliaceus creating after metastasis of cutaneous squamous cell carcinoma to regional lymph nodes. Pemphigus-like lesions induced by D-penicillamine: Analysis of clinical, histopathological, and immunofluorescence options in 34 instances. Pemphigus-like eruption induced by D-penicillamine and captopril in the same affected person. In vitro acantholysis induced by D-penicillamine, captopril, and piroxicam on dead de-epidermized dermis. Exacerbation of pemphigus foliaceus after tetanus vaccination accompanied by synthesis of auto-antibodies towards paraneoplastic pemphigus antigens. Possible mechanisms within the induction of pemphigus foliaceus by topical imiquimod remedy. D-Penicillamine-induced pemphigus foliaceus with autoantibodies to desmoglein-1 in a patient with mixed connective tissue illness. A case of penicillamine-induced pemphigus, efficiently treated by plasma change. Pemphigus foliaceus antibodies and a monoclonal antibody to desmoglein I demonstrate stratified squamous epithelial-specific epitopes of desmosomes. Pemphigus foliaceus antigen: Characterization of a keratinocyte envelope related pool and preparation of a soluble immunoreactive fragment.
Generic lisinopril 5 mg with visaCornified cell envelope proteins and keratins are normally distributed in harlequin ichthyosis heart attack in men buy cheap lisinopril 10 mg. Acquired ichthyosis: Multiple causes for an acquired generalized disturbance in desquamation blood pressure medication benicar lisinopril 10 mg generic visa. Paraneoplastic Addisonian pigmentation and bought ichthyosis as presenting features of a number of myeloma blood pressure newborn purchase 2.5 mg lisinopril visa. Acquired ichthyosis and hypertrichosis due to autoimmune thyroiditis: Therapeutic response to thyroxine alternative. Acquired ichthyosis and livedoid palmoplantar keratoderma: Two unusual pores and skin manifestations of systemic lupus erythematosus. Histopathological and, immunohistochemical evaluation of acquired ichthyosis in patients with human T-cell lymphotropic virus type 1-associated myelopathy. Mucocutaneous antagonistic effects of hydroxyurea: A prospective research of 30 psoriasis patients. Pathogenesis of abnormal keratinization in ichthyosiform cetrimide dermatitis: An ultrastructural examine. Acquired ichthyosis as a manifestation of acute cutaneous graft-versus-host illness. Pityriasis rotunda in a white affected person: Report of the second case and evaluate of the literature. Pityriasis rotunda: A cutaneous marker of hepatocellular carcinoma in South African blacks. Pityriasis rotunda as a cutaneous marker of hepatocellular carcinoma: A comparison with its prevalence in other ailments. The effectiveness of long-term dietary remedy within the remedy of grownup Refsum illness. Redefining the Sj�gren�Larsson syndrome: Atypical findings in three siblings and implications concerning diagnosis. Sj�gren�Larsson syndrome: Early prognosis, dietary management and biochemical research in two instances. The molecular foundation of Sj�gren�Larsson syndrome: Mutation analysis of the fatty aldehyde dehydrogenase gene. A novel connexin 26 mutation in a patient identified with keratitis�ichthyosis�deafness syndrome. A novel connexin 26 gene mutation related to options of the keratitis�ichthyosis�deafness syndrome and the follicular occlusion triad. Trichothiodystrophy-like hair abnormalities in a child with keratitis ichthyosis deafness syndrome. Keratitis, ichthyosis and deafness syndrome with growth of a number of hair follicle tumours. X-linked dominant Conradi�H�nermann syndrome presenting as congenital erythroderma. Ichthyosis and keratotic follicular plugs, containing dystrophic calcification in newborns: Distinctive histopathologic options of X-linked dominant chondrodysplasia punctata (Conradi�H�nermann�Happle syndrome). Clinical variation in X-linked dominant chondrodysplasia punctata (X-linked dominant ichthyosis). Usefulness of histopathologic examination of thick scales within the analysis of X-linked dominant chondrodysplasia punctata (Happle). Case of Conradi�Hunermann�Happle syndrome with alopecia: Histological examination of affected follicles. A spectrum of phenotypical expression of Neu�Laxova syndrome: Three case reviews and a evaluate of the literature. A novel X-chromosomal microdeletion encompassing congenital hemidysplasia with ichthyosiform erythroderma and limb defects. Dorfman�Chanarin syndrome in a Turkish kindred: Conductor analysis requires evaluation of a quantity of eosinophils. Neutral lipid storage leads to acylceramide deficiency, probably contributing to the pathogenesis of Dorfman�Chanarin syndrome. Ichthyosis, exocrine pancreatic insufficiency, impaired neutrophil chemotaxis, development retardation, and metaphyseal dysplasia (Shwachman syndrome). Ichthyosiform dermatosis and deafness: Report of a case and, review of the literature. Ichthyosiform erythroderma and cardiomyopathy: Report of two circumstances and evaluation of the literature. Migratory ichthyosiform dermatosis with type 2 diabetes mellitus and insulin resistance. Genetic syndrome with ichthyosis: Congenital ichthyosis, follicular atrophoderma, hypotrichosis, and woolly hair; second report. Acquired palmoplantar keratoderma and immunobullous disease associated with antibodies to desmocollin 3. Congenital ichthyosiform dermatosis with linear keratotic flexural papules and sclerosing palmoplantar keratoderma. Congenital atrichia, palmoplantar hyperkeratosis, mental retardation, and early lack of tooth in 4 siblings: A new syndrome Palmoplantar keratoderma with an unusual composition of stratum corneum and serum sterol derivatives: A new entity Two siblings born preterm with large ears and hypopigmented hair who developed palmoplantar keratoderma and frontal cranium bossing: A new syndrome Inherited palmoplantar keratoderma and sensorineural deafness related to A7445G level mutation in the mitochondrial genome. Palmoplantar keratoderma and leukokeratosis anogenitalis: the second case of a brand new disease. Palmar�plantar keratoderma of Unna Thost associated with atopic dermatitis: An underrecognized entity A mutation in the V1 finish area of keratin 1 in non-epidermolytic palmar�plantar keratoderma. Syndrome de Olmsted (keratodermia palmoplantaire, et periorificielle congenitale). Olmsted syndrome: Mutilating palmoplantar keratoderma with periorificial keratotic plaques. Olmsted syndrome: Report of a case with study of the cellular proliferation in keratoderma. Palmoplantar and perioroficial keratoderma with, corneal epithelial dysplasia: A new syndrome. Palmoplantar keratoderma and skin grafting: Postsurgical long-term follow-up of two circumstances with Olmsted syndrome. A recurrent mutation in the loricrin gene underlies the ichthyotic variant of Vohwinkel syndrome. Keratoderma hereditaria mutilans (Vohwinkel): Differentiating features of situations with constriction of digits. Keratoderma hereditaria mutilans:, Etretinate therapy and electron microscope research. Successful treatment of, keratoderma hereditaria mutilans with an fragrant retinoid. Towards characterization of palmoplantar keratoderma attributable to gain-of-function mutation in loricrin: Analysis of a household and review of the literature. Hereditary epidermolytic palmo-plantar keratoderma (V�rner type) � Report of a household and evaluate of the literature. Mutations in keratin K9 in kindreds with, epidermolytic palmoplantar keratoderma and epidemiology in Northern Ireland. A novel keratin 9 gene mutation (Met156Arg) in a Japanese patient with epidermolytic palmoplantar keratoderma. Hereditary epidermolytic palmoplantar keratoderma associated with breast and ovarian cancer in a big kindred. Ultrastructural changes ensuing from keratin-9 gene mutations in two families with epidermolytic palmoplantar keratoderma. Mutations of keratin 9 in two families with palmoplantar epidermolytic hyperkeratosis. Mutations within the 1A area of keratin 9 in sufferers with epidermolytic palmoplantar keratoderma. R162W mutation of keratin 9 in a household with autosomal dominant palmoplantar keratoderma with unique histologic options.
Discount lisinopril 5 mg with amexDyschromatosis (hyperpigmentation and hypopigmentation): dyskeratosis congenita blood pressure chart printable generic lisinopril 10 mg without a prescription, dyschromatosis symmetrica hereditaria (Dohi) arteria femoralis profunda buy lisinopril 2.5 mg on-line, dyschromatosis universalis hereditaria blood pressure levels in adults order lisinopril 5 mg visa, familial gigantic melanocytosis, heterochromia extremitarum,472 Fanconi anemia,476 and hereditary congenital hypopigmented and hyperpigmented macules. Pigment-containing melanophages are typically current within the higher dermis, significantly in black patients. Residual options of the previous or concurrent inflammatory dermatosis may be present. Hyperkeratosis was present within the lesions of a affected person with confettilike leukoderma that followed psoralen photochemotherapy;449 the hyperkeratosis has not been current in other circumstances. Alterations within the epidermal configuration also can produce apparent pigmentation of the skin. Fixed drug eruptions and dyskeratosis congenita are discussed with the lichenoid response pattern on pages fifty three and seventy seven, respectively. Histopathology Basal hyperpigmentation is the standard discovering, though a rise in basal melanocytes with related acanthosis has additionally been reported. The case of Zhang and Zhu additionally showed slight hyperkeratosis, vasodilatation, a mild perivascular lymphohistiocytic infiltrate, and pigmentary incontinence. Spontaneous resolution could be anticipated inside a number of months to a few years,497,500 although a case lasting 21 years, with several episodes of spontaneous decision adopted by recurrences, has been reported. There is a rise in melanin in the lower layers of the epidermis and typically a small amount of pigment within the dermis. Of curiosity is the discovering of huge nuclei within the keratinocytes of the pigmented pores and skin in some megaloblastic anemias. Cases from Japan, China, and Korea typically have an autosomal dominant sample of inheritance. Both dyschromatosis symmetrica hereditaria and dyschromatosis universalis hereditaria (see later) are inherited pigmentary skin issues. In the latter situation, skin lesions occur earlier (first month of life) and truncal involvement is often current, whereas the lesions in dyschromatosis symmetrica hereditaria are predominantly acral in location. They are characterised by linear, whorled, or reticulate areas of hyperpigmentation. Clinical variants have been described,527�531 and one case has been related to thrombocytopenia, hypochromic microcytic anemia, and unilateral conduction deafness. The explanation for the dysfunction is unknown, however melanocytes in each hyper- and hypopigmented pores and skin appear to be unable to ship melanin to the encircling keratinocytes. They are current in both hyper- and hypopigmented zones, but there are fewer melanocytes in the hypopigmented areas. There are areas with hyperpigmented basal cells alternating with poorly pigmented pores and skin. Pigment can also be deposited in the dermis, with a few of it residing inside melanophages. It has also been reported in ladies taking isotretinoin575 or hormone alternative therapy;576 the forearms are sometimes involved in this latter group. There is increased expression of -melanocyte-stimulating hormone in lesional skin580 and elevated expression of stem cell issue within the dermis and of its receptor c-kit within the epidermis. Histopathology589 the pigmented lesions showed epidermal atrophy, elevated basal layer pigmentation, superficial telangiectases, and actinic elastosis. On ultrastructural examination, the pigmented macules have shown increased numbers of melanosome complexes inside basilar keratinocytes. Histopathology There is elevated melanin in the epidermis, particularly in the basal layers. Melanin is increased within the basal layers of the dermis, however melanocytes are normal in quantity and morphology. The outline of the macules could be very irregular, in contrast to that of caf�-au-lait spots. However, quantitative research have proven a slight improve in melanocytes, that are accommodated in focally elongated rete ridges. The prevalence of a hypocellular marrow in a single patient may have been a fortuitous affiliation. The most common malignancies, so as of frequency, are colorectal, breast, small bowel, gastric, and pancreatic. Lesional tissue has been found to have an elevated stage of androgen receptors, suggesting that heightened local androgen sensitivity may result in the hypertrichosis. Q-switched lasers are utilized in pigmented variants, but a number of treatments are essential. There is variable hyperpigmentation of the basal layer with some melanophages within the dermis. Melanocyte proliferation is usually mild and not at all times obvious in routine sections; special research have proven a quantitative improve. There are conflicting views regarding whether or not the melanocytes are quantitatively elevated. In the hypopigmented macules, there have been additionally filiform downgrowths of the epidermis; with Fontana� Masson staining, pigmentation was limited to the ideas of rete ridges, with lack of pigment in the the rest of the basilar layer. In Galli�Galli illness, there are digitate downgrowths of the rete ridges with basal hyperpigmentation. There are suprabasal acantholytic lacunae with a slightly parakeratotic roof however no significant dyskeratosis. This lesion reveals elevated amounts of melanin in the basal layer, in addition to prominent melanin incontinence. The repigmentation observed in lichen sclerosus, following using topical tacrolimus, concerned basal hyperpigmentation and not melanin incontinence. There can also be occasional lymphocytes round vessels in the papillary dermis and a gentle increase in fibroblasts and even collagen in the papillary dermis. There is often no evidence of the underlying dermatosis that resulted in the space of pigmentation. Electronmicroscopy Melanosomes are markedly elevated in keratinocytes, and these could also be dispersed by way of the cytoplasm or loosely aggregated. Prominent hyperpigmentation is nearly invariable in the resolving phases of a phytophotodermatitis (see p. A scant perivascular infiltrate of lymphocytes and typically plasma cells may be current. Other reported findings include the absence of dermatoglyphics, hypohidrosis or hyperhidrosis, hyperkeratosis of palms and soles, and nonscarring acral blisters. Another reported case showed basal layer degeneration, dermal melanophages, and an absence of appendages. There are delicate interface changes with some vacuolar change and apoptotic keratinocytes. This is followed by neutrophilic spongiosis and focal epidermal microabscesses, accompanied by ballooning and degeneration (both apoptotic and necrotic) of keratinocytes. This is quickly adopted by the influx of eosinophils and lymphocytes into the upper dermis. This microscopic description is principally in settlement with a study of 50 instances by Kim et al. In the third stage, which has a peak onset at approximately 3�6 months, there are streaks and whorls of brown to slate grey pigmentation, typically asymmetrically distributed on the trunk and typically on the extremities. Areas of hyperpigmentation, typically related to verrucous plaques, could remain. There are occasional dyskeratotic cells with eosinophilic hyaline cytoplasm in the epidermis adjacent to the vesicles. Some macrophages migrate into the dermis; on electron microscopy, these have been shown to phagocytose the dyskeratotic cells as nicely as melanosomes. Pale scarred areas could additionally be found on the lower part of the legs; these present a reduction within the number of melanocytes and a few increase in dermal collagen. Note that there are additionally a couple of remnant dyskeratotic cells at the epidermal surface (arrows). There are quite a few melanophages, particularly round vessels within the superficial plexus.
Discount lisinopril 2.5 mg visaProtruding into the lacuna are villi hypertension 30 year old male cheap lisinopril 5 mg on-line, that are dermal papillae lined by a layer of basal cells blood pressure chart on age lisinopril 2.5 mg buy discount. The papillae comprise dilated vessels heart attack symptoms in men 5 mg lisinopril discount mastercard, occasional Differential prognosis the differential diagnosis of Hailey�Hailey illness consists of other acantholytic dermatoses, an important of which is pemphigus. Although each disorders present suprabasilar acantholysis, the diploma of acantholysis tends to be a lot greater in Hailey�Hailey disease, whereas in pemphigus, often only a few acantholytic cells are normally evident within the blister cavity. The latter tends to occur in middle-aged sufferers as scaly papules, significantly over the trunk. However, the small, self-limited nature of the lesions would ordinarily permit a assured diagnosis. A further consideration is the entity acantholytic dermatosis of the genitocrural region (papular acantholytic dyskeratosis). A cup-shaped invagination is filled with a keratinous plug that in flip overlies an space of suprabasal clefting. In a examine of forty six warty dyskeratomas accessioned in Graz, Austria, three patterns had been discerned on scanning magnification. It is analogous to different epithelial patterns of disordered keratinization similar to epidermolytic hyperkeratosis and acantholytic dyskeratosis. The following prospects were thought-about in the authentic article: a variant of epidermolytic hyperkeratosis, a variant of maturation in a verruca vulgaris, or a variant of the epidermolytic-like adjustments seen in ichthyosis hystrix of Curth� Macklin and associated issues (see p. Overlying the thickened granular layer, at the tips of the epidermal papillations, are orthokeratotic mounds of huge, eosinophilic corneocytes. There is commonly some basket-weave orthokeratin overlying thick and compacted orthokeratin. A pale basophilic substance is present in the larger spinous layer and granular zone. In addition, stains for cytokeratins 7 and 20 are adverse in the cells of pagetoid dyskeratosis. Discrete keratotic lesions related to palmar�plantar involvement or cornoid lamellation are thought-about elsewhere on this chapter. Certain acquired lesions such as warts, cutaneous horns, callosities, corns, stucco keratoses, solar keratoses, seborrheic keratoses, and lesions produced by tar could current as discrete keratotic lesions. It seems to outcome from a defect in keratinization with the buildup of cytokeratin precursors or associated protein products. Several stories, but not all,1375,1378 have documented a decrease in or qualitative defects of the membrane-coating granules (lamellar or Odland bodies) in affected areas of dermis. In old lesions, the epidermal atrophy is now not present and the inflammatory infiltrate within the upper dermis is absent. If serial sections are studied, a focus the place the epidermal cells are absent and the keratotic plug is in touch with the dermis will often be seen. An Electron microscopy Studies have proven a discount in keratohyaline granules and a few persistence of desmosomal parts within the stratum corneum. There is a keratin plug overlying an invaginated, atrophic dermis (that truly represents a follicular infundibulum in this case). The plug contains parakeratosis and degenerated connective tissue and cellular debris. Transepidermal elimination may be identified at the base of the lesion on the proper (arrow). Eccrine duct involvement was present in one atypical case reported in the literature. Generalized types embody a quantity of minute digitate hyperkeratosis (nonfollicular), lichen spinulosus, and phrynoderma (follicular). Localized forms include spiny keratoderma, arsenical keratosis, and multiple filiform verrucae (palmoplantar); post-irradiation digitate keratosis; and hyperkeratotic spicules, trichodysplasia spinulosa, and multiple filiform verrucae (facial). Histopathology the spicules are composed of densely compacted, thin stacks of orthokeratotic material, typically arising from a finely pointed epidermal elevation. The digitate keratoses that develop following irradiation are characterised by parakeratotic plugs and underlying epidermal invaginations. It can occur in four completely different medical settings: a familial sort with autosomal dominant inheritance,1409�1413 a sporadic type,1413�1415 a paraneoplastic variant,1416 and a postinflammatory sort. Cases localized to the palms and soles (spiny keratoderma, palmar filiform hyperkeratosis,1419 and music-box spine keratoderma) are in all probability best Electron microscopy Electron microscopy exhibits a thickened stratum corneum and a reduced keratohyalin content within the superficial dermis. There Histopathology Waxy keratoses of childhood are characterized by marked orthokeratotic hyperkeratosis, tenting/papillomatosis of the epidermis, and some acanthosis. There is some resemblance to confluent and reticulated papillomatosis (Gougerot and Carteaud) (see p. There is compact orthokeratosis and low papillomatosis imparting an undulating appearance to the epidermis. Similar findings were reported in two of the beforehand talked about patients with acrokeratosis verruciformis having the P602L mutation. The earliest adjustments in xeroderma pigmentosum normally develop before the age of 2 years with a extreme sunburn response and the event of a number of freckles with variable intensity of melanin pigmentation and interspersed hypopigmented macules. Skin tumors, which embrace photo voltaic keratoses, cutaneous horns, keratoacanthomas, squamous and basal cell carcinomas, basosquamous carcinoma, atypical fibroxanthoma,1469 malignant melanomas,1470 and angiomas, may develop in late childhood; sufferers might ultimately die from the consequences of their tumors. In one research, a skin fibroblast cell strain from a affected person with xeroderma pigmentosum was reported to have proven spontaneous morphological transformation to an anchorage-independent form after serial passage. This abnormality is also present in keratinocytes and melanocytes cultured from affected patients. They are actually categorised on the basis of the presence or absence of trichodysplasia,1529 dental abnormalities, onychodysplasia, and dyshidrosis. It contains reticulate pigmentation of the skin as an necessary element and is subsequently mentioned with different problems of pigmentation (see p. The gene maps to chromosome 17q21 in the region of the kind 1 keratin gene cluster. Most of the syndromes are extremely rare and of little dermatopathological significance. At least 20 mutations of this gene exist, resulting in a unique clinical severity for each mutation group. There could also be variability in epidermal melanin concentration, telangiectasia of superficial vessels, and a mild perivascular inflammatory cell response. With time, the pigmentary adjustments are extra marked, with areas of distinguished melanin pigmentation of the basal, malpighian, and spinous layers and pigmentary incontinence. There is finally distinguished photo voltaic elastosis and the development of areas of hyperkeratosis. A case with hemihidrosis has been reported, indicating that this syndrome, though not normally included with the ectodermal dysplasias, does meet the standards for this category of illnesses. Vegetative, hyperkeratotic plaques develop over the oral commissures and the mid-portions of the lips. Eccrine glands are absent or rudimentary, although poorly shaped intraepidermal eccrine ducts could additionally be current. There is a reduction in pilosebaceous follicles, though, paradoxically, foci of sebaceous hyperplasia have sometimes been noted on the higher cheeks. The sweat glands are also normal in quantity in the orofaciodigital syndrome, however sebaceous glands are diminished or absent. No specific histological options have been described in the cardiofaciocutaneous syndrome. In ectodermal dysplasias with clefting, the pilosebaceous follicles are reduced in size and small vellus follicles are present. Findings embody focal hyperkeratosis, papillomatosis, and acanthosis with marked elongation of the rete ridges. Cryotherapy and topical keratolytics have been used, however brokers similar to 40% urea, 12% lactic acid lotion, and topical retinoids have given combined or poor results. These changes are seen in localized and type A generalized forms of peeling skin syndrome. A case of granular parakeratosis of eccrine ostia introduced with small pruritic papules on the face and neck,1667 and one other case displayed brownish verrucous papules on the neck.
Lisinopril 2.5 mg buy cheap on lineIdentification of a causative mutation in one of the three fibrinogen genes will verify the diagnosis pulse pressure chart 2.5 mg lisinopril cheap overnight delivery. The standard remedy is on demand blood pressure 50 order lisinopril 5 mg amex, in which fibrinogen is run as quickly as potential after onset of bleeding blood pressure medication diltiazem purchase 2.5 mg lisinopril mastercard. Another strategy is major prophylaxis that features administration of fibrinogen concentrates from an early age to forestall bleeding and, in the case of pregnancy, to forestall miscarriage. Effective long-term secondary prophylaxis with administration of fibrinogen every 7 to 14 days (particularly after central nervous system bleeds) has been advocated. The frequency and dose of fibrinogen concentrates should be adjusted to maintain a level above 0. According to these guidelines, in case of bleeding fibrinogen levels should be increased to 1. To increase the fibrinogen focus of 1 g L-1, a dose of approximately 50 mg/kg is required. Women with congenital afibrinogenemia are capable of conceive and embryonic implantation is normal, however the being pregnant normally results in spontaneous abortion at 5 to eight weeks of gestation until fibrinogen alternative is given. Continuous infusion of fibrinogen focus must be carried out during labor to keep fibrinogen greater than 1. Available Treatments and Modalities Genotype�Phenotype Correlations: Potential Importance of Global Assays Current diagnostic checks are acceptable for establishing the prognosis but clearly extra checks are required for a more correct prediction of the scientific phenotype of a patient and consequently the appropriate treatment. Indeed, though in afibrinogenemia all patients have unmeasurable functional fibrinogen, the severity of bleeding is highly variable amongst sufferers, even amongst these with the same genotype. One potential explanation for the noticed variability of medical manifestations is the existence of modifier genes/alleles: some variants might increase the severity of bleeding while others may ameliorate the phenotype. The existence of modifying genes/ polymorphisms can additionally be strongly suspected within the beforehand discussed instances of hypofibrinogenemia associated with fibrinogen inclusion our bodies in hepatocytes. Chapter a hundred twenty five: Hereditary Fibrinogen Abnormalities 2157 In addition to fibrinogen substitution, antifibrinolytic brokers could also be given, particularly to treat mucosal bleeding or to forestall bleeding following procedures such as dental extraction. Fibrin glue is useful to treat superficial wounds or following dental extractions. Oral iron preparations may be given in cases with associated iron-deficiency anemia. Routine vaccination against hepatitis, as nicely as a regular surveillance for both the illness and treatment-related problems in a complete care setting, is extremely really helpful. Most affected patients are heterozygous for missense mutations within the coding region of one of many three fibrinogen genes. There can also be a risk of transfusion-related acute lung injury, because of the presence of cytotoxic antibodies within the infused plasma. Acquired inhibitors to fibrinogen after alternative remedy have been reported in only two cases. One rationalization for some circumstances is that minute quantities of fibrinogen, which can only be detected by extremely sensitive immunoassays, are present in the circulation. One of the main problems in afibrinogenemic patients is thrombosis, which may happen spontaneously following blood part remedy. Successful use of lepirudin has been reported for an afibrinogenemic affected person who suffered recurrent arterial thrombosis regardless of therapy with heparin and aspirin. New Preparations the growing need for fibrinogen preparations in congenital but additionally in acquired deficiencies has stimulated some firms to enhance present preparations or to develop new ones. Dysfibrinogenemia is outlined by the presence of regular levels of functionally irregular plasma fibrinogen. As in afibrinogenemia and hypofibrinogenemia, each are heterogeneous issues attributable to variations in clots fashioned from dysfibrinogens. Control clot from normal purified fibrinogen clotted with thrombin displaying comparatively uniform distribution of fibers forming a branched network. Clot from fibrinogen Caracas I96 displaying very skinny fibers, indicating a defect in lateral aggregation. The described mutants are fairly often named after the town of origin of the family or the town of the laboratory characterizing the mutation. Many instances are asymptomatic and are solely identified because of routine coagulation screening. Indeed, a compilation of approximately 250 cases revealed that fifty five percent of sufferers have been asymptomatic, 25 percent had a historical past of bleeding, and 20 %, an inclination towards thrombosis. Most of those cases are asymptomatic, however some patients heterozygous for R301C (R275C) have thrombophilia, typically in affiliation with an extra thrombotic danger issue corresponding to factor V Leiden. Other substitutions involving residue R38 (R19) have been discovered to be related to bleeding in some cases, for example, Munich I, R38N (R19N), and Mannheim I, R38G (R19G), and with thrombosis in different cases, for instance, Aarhus and Kumamoto, which are also a results of R38G (R19G). The mechanism for thrombophilia remains unclear, however coexisting threat elements may contribute to the scientific manifestations. Furthermore, the inability of a mutant fibrin to successfully bind and sequester thrombin might play a job in such a medical presentation. Bleeding that occurs underneath situations involving defective fibrinopeptide release or manufacturing of a defective "A" knob is most probably related to the reduced polymerization potential of the mutant fibrins which are produced, with resulting faulty clot formation. Mutations Resulting in Abnormal "A" Knobs or Deficient Fibrinopeptide Release Hypodysfibrinogenemia which is outlined by low levels of a dysfunctional protein may be brought on by different molecular mechanisms. A compilation of greater than 260 instances of dysfibrinogenemia revealed that fifty five p.c of the sufferers had no medical problems while 25 p.c exhibited bleeding, and 20 % had a bent to thrombosis, mainly venous. Some mutations in the A chain of fibrinogen are related to a particular form of hereditary amyloidosis. However, steady fibrinogen-related amyloid deposition in the end ends in allograft destruction. Combined liver and kidney transplantation prevents additional amyloid deposition in the renal allograft and elsewhere but is associated with additional perioperative and subsequent risks. Mutations Leading to Polymerization Defects in the D Region Sites within the D region essential for fibrin polymerization are affected in plenty of dysfibrinogenemias. Dysfibrinogenemia is recognized by a discrepancy between clottable and immunoreactive fibrinogen. However, even in specialized laboratories, this analysis can be tough as a outcome of the sensitivity of the checks depends on the particular mutation, reagents, and methods. The dedication of the precise nature of a fibrinogen defect has to be performed in extremely specialised laboratories since it includes purification of fibrinogen, measurement of the speed of fibrinopeptide cleavage, evaluation of fibrin monomer polymerization, and fibrinolysis. Thromboelastography, generally used for choice making for fibrinolytic and anticoagulant remedy, may be notably useful for investigation of dysfibrinogenemia. The thromboelastography signal is fibrin dependant, its amplitude is enhanced by platelets and reflects the stretch and restoration of the clot during its formation. In addition, there are a quantity of case stories of acquired dysfibrinogenemia secondary to pancreatitis, paraneoplastic syndrome, and renal carcinoma. The acquired dysfibrinogenemias characterize a heterogeneous group of disorders with multiple pathogenetic mechanisms, essentially the most clearly defined fibrinogen abnormalities being an increase in carbohydrate content in patients with liver disease. These irregular fibrinogens are usually characterised by extended thrombin and reptilase times, by abnormal fibrin monomer polymerization however with regular fibrinopeptide release. In some circumstances no underlying illness is discovered, and to decide whether a fibrinogen abnormality is congenital or acquired may be tough. The demonstration of the identical fibrinogen abnormality in another family member is a robust argument for a congenital dysfunction. When measured in newborns, fibrinogen ranges must be interpreted with caution as a result of neonatal fibrinogen has an altered content material of carbohydrate that may mimic dysfibrinogenemia in certain laboratory checks. Rare circumstances of circulating autoantibodies to fibrinogen, for example in systemic lupus erythematosus and in sufferers receiving surgical sealants containing bovine fibrinogen, have also been reported. Genotype Analysis the gold normal for the analysis of dysfibrinogenemia is the characterization of the molecular defect. In our recent study of 101 dysfibrinogenemia circumstances,76 87 percent of the causative mutations were positioned in these two exons. Indeed, as already discussed, subjects with hereditary dysfibrinogenemias may be asymptomatic throughout their entire life or may endure from bleeding and/or thrombotic problems. Topical fibrin glue or antifibrinolytic brokers may be used for superficial bleeds. |







